By KFF Health News’ Arielle Zionts
Mont. EKALAKA. In early June, a patient arrived at the emergency room of the little hospital at the crossroads of two dirt roads in this 400-person hamlet, but there was no doctor on duty.
It never is.
Instead, Dahl Memorial’s three-bed emergency room, which is two hours away from the nearest hospital with more sophisticated facilities, relies on nurse practitioners and physician assistants.
Even with a doctor there, Carla Dowdy, a physician assistant, recognized that the patient required more care than the emergency room could offer. In order to transport the patient to therapy at Montana’s most cutting-edge hospital, she called for a medical plane. As a paramedic and nurses gave the meds, put IV lines in, and took vital signs, Dowdy also shouted out the medications and dosages required to stabilize the patient.
In the midst of a national physician shortage, emergency rooms, particularly those in rural areas, are increasingly run with few or no doctors, according to emergency care academics and providers.
According to a recent study, at least 7.4% of emergency rooms in the United States lacked a doctor on duty around-the-clock in 2022. Similar to Dahl Memorial, over 90% were located in critical access or low-volume hospitals, which are classified by the federal government as tiny, rural hospitals.
A poll that was issued to all emergency rooms in the nation—aside from those run by the federal government—received responses from 82% of hospitals. Carlos Camargo, the lead author and an emergency medicine professor at Harvard Medical School, stated that as the study is the first of its sort, there is no evidence that such staffing arrangements are becoming more common. However, Camargo and other specialists believe that emergency rooms operating without medical personnel are growing increasingly frequent.
Giving ERs to non-physicians is not without criticism. According to some medical professionals and their associations, hospitals are merely trying to save money by not hiring doctors since they believe that their rigorous training results in better service.
Both the American College of Emergency Physicians and the American Medical Association, which is open to all doctors and medical students, favor state and federal laws or rules that would mandate that emergency rooms have a doctor on site at all times. Such laws were recently passed in South Carolina, Virginia, and Indiana.
According to ACEP president Alison Haddock, rural emergency rooms may see fewer patients, but they nevertheless handle catastrophic cases.
According to Haddock, it’s critical that residents in those locations have as much equal access as possible to high-quality emergency treatment.
According to other medical professionals and organizations, advanced practice clinicians may manage emergency rooms if they have the necessary training and assistance. Additionally, they claim that requiring a doctor to be present on-site may force some rural hospitals to close because they are unable to pay for or hire enough doctors.
According to Paul Amiott, a board member of the Society of Emergency Medicine PAs, it works effectively in an environment, particularly a rural one, provided you have an experienced PA who understands what they know, knows when to involve experts, and knows the bounds of their knowledge.
“I work 12-hour night shifts at critical access hospitals in three states without physicians on site, but I’m not practicing independently,” he claimed.
According to Amiott, he frequently consults with specialists and, once a month or so, requests assistance from the hospital’s day shift doctor in handling more difficult cases like complex trauma and emergency deliveries. According to Amiott, this isn’t exclusive to PAs; ER physicians also seek comparable assistance and consultations.
States differ greatly in the percentage of emergency rooms that do not always have an attending physician on site. According to the 2022 poll, there were no such emergency departments in 15 states, including several that were largely rural, such West Virginia, Nevada, and New Mexico.
However, over half of the EDs in the Dakotas were operating without a physician on duty around-the-clock. Montana had the third-highest rate, at 46%.
There isn’t a program in any of those three states that trains doctors to be emergency room specialists. Idaho and Wyoming don’t either.
Sanford Health, however, is starting an emergency medical residency in the area. The organization claims to be the biggest rural health system in the US. According to a news release from the residency director, the program, which is situated in Sioux Falls, South Dakota, aims to increase the number of rural emergency physicians in those states.
Leon Adelman practices emergency care in Gillette, Wyoming, the largest city in the northeastern part of the state with over 33,800 population. He has developed complex opinions about whether states should mandate round-the-clock on-site physician care in emergency rooms as a result of working in such a remote location.
According to Adelman, he only favors such legislation in states where they are practical, such as Virginia. He claimed that only after conducting research that gave them confidence that the requirement wouldn’t force any rural hospitals to close did the state’s emergency physicians organization advocate for the law.
According to Camargo, some physicians argue that hospitals should be compensated to assist in implementing 24/7 on-site physician care in emergency rooms if politicians are going to mandate it.
According to Adelman, states ought to establish alternative regulations in cases where enforcing staffing levels is not feasible. He stated, for instance, that lawmakers should ensure that hospitals that do not hire doctors are not doing it merely to save money.
Related Articles
-
US pediatricians new COVID-19 shot recommendations differ from CDC advice
-
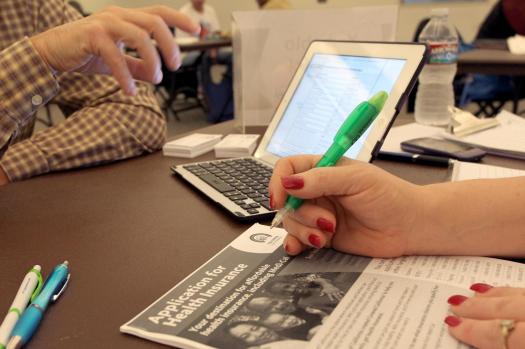
Even in states that fought Obamacare, Trump s new law poses health consequences
-
Texas declares measles outbreak over
-
FDA s new expert panels are rife with financial conflicts and fringe views
-
AI eroded doctors ability to spot cancer within months in study
He cited a research that suggested numerous hospitals in the state of Vermont remove doctors from their emergency rooms. A mandated process to repair the state’s dysfunctional health care system included the study.
According to Adelman, states ought to mandate that PAs and NPs who do not have on-site physician supervision possess substantial emergency expertise and the capacity to consult with physicians remotely.
Some medical professionals have cited a case in which a 19-year-old woman passed away following a misdiagnosis made by a nurse practitioner (NP) who worked alone in an emergency room in Oklahoma and was qualified in family medicine rather than emergency care. According to an investigation, few NPs are certified in emergency situations.
Training and experience are outlined by the Society of Emergency Medicine PAs.PAs must to have prior experience working in remote locations or without doctors on staff.
Emergency physicians have observed instances of hospitals using unskilled advanced-practice providers, according to Haddock. According to her, ACEP is requesting that the federal government mandate that rural emergency hospitals and critical access hospitals have doctors on staff or available for calls around-the-clock.
Haddock stated that ACEP has several initiatives to maintain the funding and staffing of rural hospitals and stated that the group would not want such a requirement to close any hospitals.
According to Dowdy, who spent 14 years working in busy metropolitan emergency departments, Dahl Memorial Hospital has stringent hiring standards and strong oversight.
“A doctor who lives on the other side of Montana reviews all their patient treatment notes,” she said, adding that emergency room workers can phone doctors with questions. According to Dowdy, the emergency room is working on virtual reality glasses that will enable distant doctors to assist by viewing what the Ekalaka professionals see.
According to her, the Ekalaka ER sees an average of one or two patients each day, which is insufficient for staff to keep up their expertise. Providers do monthly simulated scenarios, visit simulation labs, and practice advanced skills like guiding breathing tubes into patient airways with an ultrasound to augment those real-life cases.
Dahl Memorial hasn’t had a doctor in at least 30 years, according to Dowdy, although CEO Darrell Messersmith stated that if a doctor lived nearby, he would recruit one. Having advanced-practice physicians who have ties to the area and who remain at the hospital for a number of years has advantages, according to Messersmith. He pointed out that doctors at other remote hospitals can be contract employees who come in for a few weeks at a time or permanent employees who depart after a few years.
People who visited the hospital’s clinic and dined at Ekalaka’s only breakfast establishment told KFF Health News that they were pleased with the treatment they received from Dowdy and her colleagues.
A cow on Ben Bruski’s family ranch kicked a fence, shattering it against his hand, forcing him to go to the emergency room. Additionally, he is aware of other individuals who have received treatment for more severe issues.
“This facility is essential because it saves a lot of lives,” Bruski stated.
KFF Health News, 2025. Tribune Content Agency, LLC is the distributor.